About 1,500 Days and Counting . . . (Part I)

It has been about 4 years since the world became addicted to Pandemic Porn and went a little Chinese bat (shit) crazy.

What I want to do is to provide a summary (although it will be a long one) of what happened, or at least my best current assessment of what happened, because there are profound disagreements.
The Virus
There are, very broadly speaking, 4 main camps :
Sars-Cov-2 was real and gave rise to a severe and deadly pandemic
Sars-Cov-2 was real and gave rise to an outbreak of a disease of moderate severity
There was no new virus and it was all just ‘re-badged’ flu, or similar
Viruses don’t exist anyway, so how could something called Sars-Cov-2 be the cause?
Of these 4, I think the second is by far and away the hypothesis that best fits the available data.
We shouldn’t, of course, be using anecdotal evidence to make any grand claims, but the anecdotal case for something ‘unusual’ occurring, at a time of year (in the UK) when respiratory viruses are not usually a problem, is quite strong strong, I believe.
Even within my own fairly limited circle of acquaintances it was obvious something untoward was happening.
My brother got sick, very sick, during the Summer months of 2020. My daughter’s 25-year old friend from university died of something classed as ‘covid’. A family member is an ICU nurse who witnessed severe covid illness at first hand (and hasn’t witnessed it as much since). The healthy 30-ish guy, a fitness enthusiast, who makes sure my ailing computer still works spent 2 weeks in hospital knocking on death’s door.
These slivers of anecdotal evidence are not unique. Just as thousands know someone who was badly affected by the vaccines, thousands know someone who was badly affected by covid.
The main point is that there was an actual illness. We can argue about the cause of that, say that the observed spike in deaths occurred because of medical mismanagement, but it’s hard to argue with the fact that people were getting ill. In the UK this occurred at a time when we do not expect a surge in respiratory ailments, let alone deaths. Respiratory viruses are almost always strongly affected by seasonality.
Even if we believe all the deaths to be iatrogenic in nature, largely due to mismanagement1 it is pertinent to ask what, precisely, were they mismanaging? Did they just take some perfectly healthy person and shove an intubation tube down their throat, or dose them up with midazolam? Of course they didn’t - they didn’t treat people for no reason whatsoever.
It has been argued that Sars-Cov-2 did not cause any ‘unique’ symptoms and so the evidence for the existence of a new pathogen is weak. The problem with this is that the body only produces a fairly limited range of ‘symptoms’ in response to a disease. Many symptoms arise as a product of the body’s own aggressive attempts to kill the invading pathogen. Substantial overlap of symptoms is expected and normal, particularly in the case or respiratory infections - and is the reason why things like differential diagnoses are important.
Requiring a ‘unique’ set of symptoms to characterize covid is, from the outset, problematic, shall we say. We all know, anecdotally, when a cold is ‘doing the rounds’, but we also know that not everyone gets precisely the same set of symptoms as a result.
Around Christmas time last year me and the offspring went to a family gathering in which one person was recovering from a bout of seasonal sniffles. Sure enough, 2-3 days later, me and the offspring all came down with some form of the sniffles. Similar, but not identical, symptoms were a result.
The doctor who treated my brother’s covid (one of several) was adamant that, whilst there was considerable overlap with flu-like illnesses, what he was seeing in his most serious patients was definitely not the flu. He was visibly distressed and upset at not knowing how to properly treat these patients.
So the main thing that needs explaining by any hypothesis is why so many people (in the UK) were becoming quite ill at a time of the year when we do not expect such illnesses. Forget deaths, forget tests, forget all the medical mismanagement, forget all the absurd interventions, what was causing this surge in illness?
This is the basic fact we need to address; why were people getting ill in such large numbers?
I don’t think there is any tenable hypothesis other than the circulation of a (relatively) novel viral pathogen that can properly explain this.
One argument that crops up is that the illnesses (and deaths) only occurred after the ‘pandemic’ had been declared and that Sars-Cov-2 was circulating in the population well before this with no discernible consequence until the panic button had been pushed. This is true, but overlooks the fact that viruses can do this sort of thing; they can twiddle their viral thumbs in the background and then suddenly ‘trigger’ out of seemingly nowhere. We do not know why this happens. We don’t even properly understand seasonality. Nor do we understand, in full, the mechanisms of transmission2.
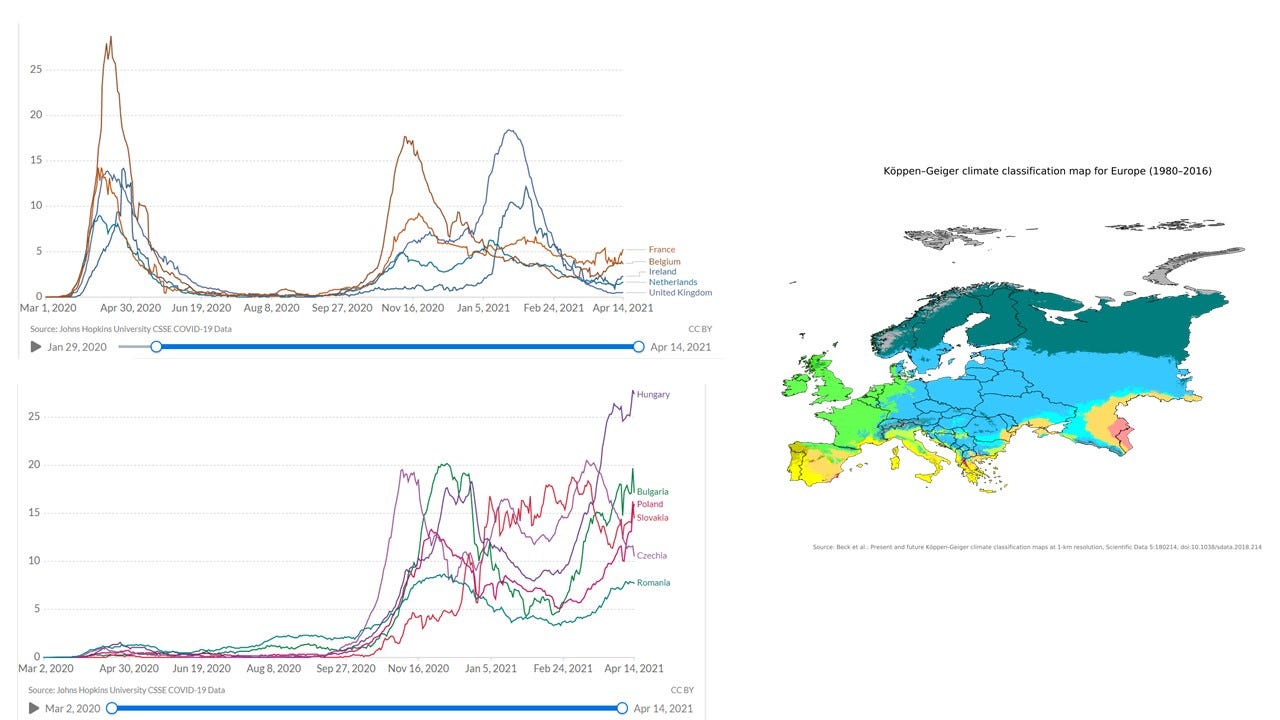
Indeed, if pushing the panic button “caused” the pandemic we must explain why certain countries, located in specific climatic regions of Europe, had a significant delay in this supposedly causal process. In some cases, things only started to get bad some months after the panic button had been pushed.
These gaps in our knowledge do not mean the virus picture is wrong - just that there are features about how it all works that we do not have the complete chapter and verse on. Until we do have a more complete picture regarding these kinds of things it’s probably best not to rely too much on simplistic and mechanistic models.
How Bad Was It?
I know that some of you will have already disagreed with my assessment on the cause of the whole covid farce but, irrespective of the cause, we need to make an assessment of the severity (of whatever it was).
One interesting statistic that was bandied about3 was that the median age of covid death in the UK was higher than median life expectancy. Fantastic - so, getting covid increased your lifespan. Best get all those grannies into the packed super-spreader nightclubs then.
I’m not being serious here (could you tell?). But we were encouraged to think of the wrinklies, particularly those of the female persuasion. Don’t kill granny became a kind of mantra.
They were right to emphasize the threat to the elderly. But at more advanced stages of life even getting a cold can be more of a risk.
The relentless Pandemic Porn that was pumped out by the media surpassed even the “white man bad” level of psyop4. People were scared for Granny, but they also became scared for themselves. But were they justified in that fear?
For the moment I’m just going to take the official UK data at face value. More on this later. What does the official data indicate for the first year of covid?
I’ve posted this chart I created before. It gives an estimate of the covid IFR (infection fatality rate) for different ages in England & Wales based on the official data from the ONS (Office of National Statistics). In order to generate this estimate I assumed an age-independent infection rate and an overall IFR for the total population. You can then work out what the IFR has to be for the different age groups based on the official figures.
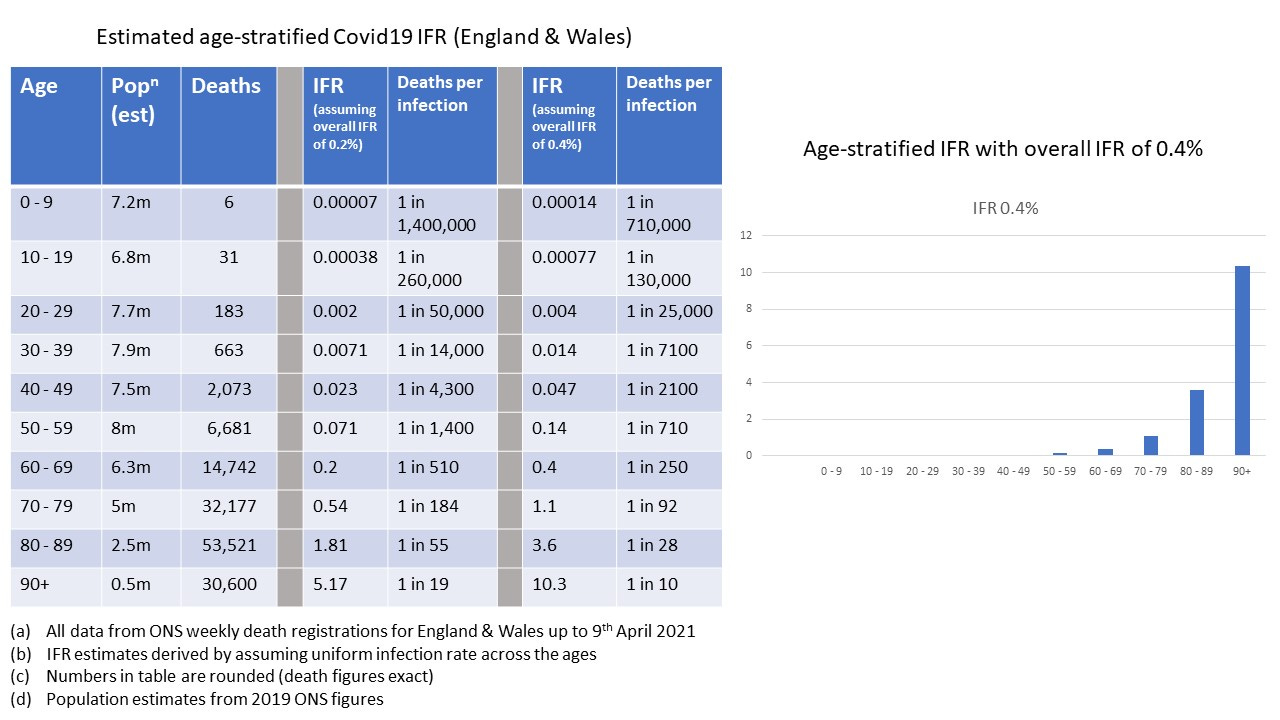
The first thing to note is that the official figures of covid deaths are overestimates, because of the way that a ‘covid’ death was classified. This means that the age-stratified IFR’s in this chart are also overestimates. It is tempting to think of them as upper bounds, but these estimates depend on the assumption made of a uniform age-independent infection rate which may not be true.
If we take the IFR as a measure of risk, then we can see that catching covid represents a very different risk between young and old; several orders of magnitude difference.
Of the 183 young people in the age bracket 20 - 29 (of which there are estimated to be 7.7 million of them) who died, ostensibly of covid, in this first year of covid in England & Wales, my daughter knew one of them. 183 out of a total of 7.7 million. It does not seem reasonable, therefore, that people in their twenties should have “lost their shit” over covid, so to speak.
We now know that the actual overall IFR of covid was less than 0.4% and almost certainly less than 0.2%. It’s interesting that the official data above for England & Wales is actually inconsistent with the assumption of an overall IFR of 0.2%. This is because of the wilful over-counting of ‘covid’ deaths that occurred.
By looking at the cumulative percentages of covid death (taken as a percentage of total covid death) we can see that the under-50 age group were not at huge risk. The upper bound estimate of IFR for the under-50 age group, based on the official death data, is about 0.0135%, or 1 death in every 7,400 infections.
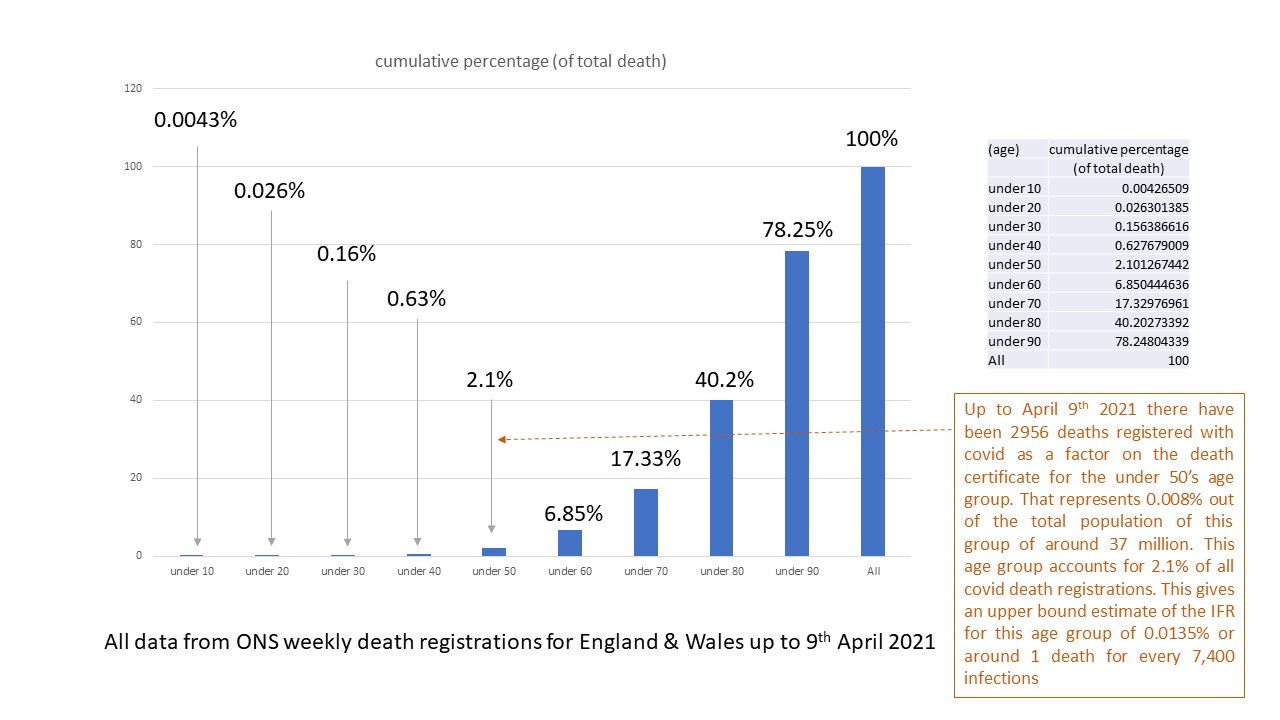
Another factor is that these estimates are all based on the 2019 estimates of population from the ONS which are likely to be underestimates. This underestimation also works to give us an overestimated IFR for the age groups.
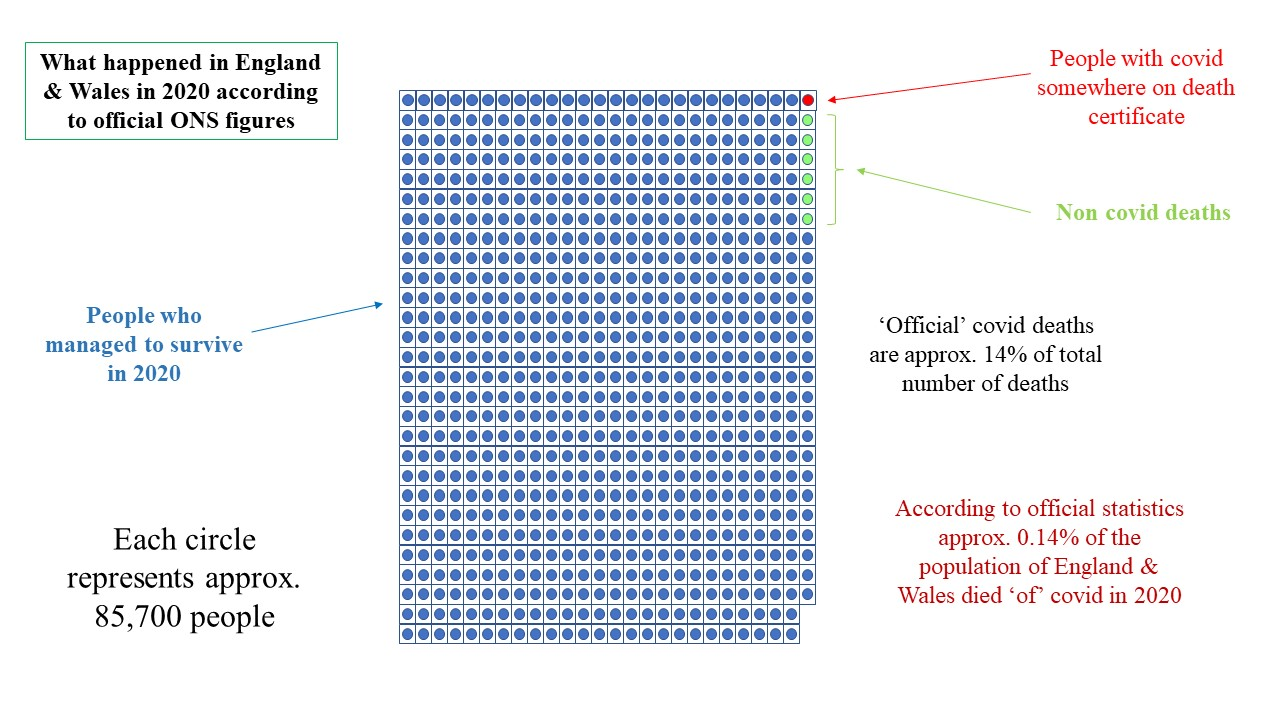
Another way to immediately visually see the overall impact of covid is to look at the total population and total deaths. Here’s a chart I created to see this (the deaths here are just from 2020 and do not extend to April 2021 as in the previous charts)
Now, all of these charts represent things that were happening during the first year of covid. This is the time when, based on the assumption that we were dealing with a novel(ish) pathogen, the population would be most at risk.
As more people become infected and survive, the disease-acquired immunity ramps up, and fewer and fewer people will be at risk. This also has a secondary effect in that, whilst possible, re-infections with covid were relatively rare5 during this period. This, therefore, would have generated a considerable degree of community protection. In crude terms, the virus was, in the words of Meatloaf, all revved up with nowhere to go.
This may not be the much-touted full ‘herd immunity’ that was so derided by the press and various Experts™, but it was a significant protective factor at a population level.
If we take the case of the measles vaccination campaign in the US in the 1960’s we can think of vaccination (live virus, attenuated) as an example of this kind of community protection. People were infected, via vaccination, with a benign form of the virus and with only 60% coverage, with a wild virus that is about 6 times more contagious than covid, it was observed that the incidence of measles cases in the US underwent a massive decline within a year.
This is a result of the fact that 60% of the population were now protected at a personal level, but also a result of the fact that should an unvaccinated person become infected then the virus had far fewer onward paths to take. This secondary effect is what massively damped down the level of observed cases.
Measles and covid are a bit different, though. Exposure to the measles virus confers lifelong subsequent immunity whereas exposure to coronaviruses, typically, does not. Earlier experiments with coronaviruses (which were of the type to lead to ‘common cold’ symptoms) had shown that re-infection was possible, although difficult and rare, and also typically led to much milder symptoms second time around.
I have read that infection with a coronavirus typically confers immunity for a period of around 2 years during which re-infection with the same virus is very unlikely.
It is difficult to look at the official data, as egregiously overestimated as it is, and to conclude that we were facing an “unprecedented” event, that constituted a health “emergency”, for which our entire system of dealing with pandemics would require revision at a global level, and that our societies would need to be re-shaped to “build back better”.
I’m not sure I would class covid quite as high as a moderate threat (overall) but one thing’s absolutely 100% certain - it was not the deadly, unprecedented, health emergency that we were continually told it was.
The figures in the US seem to have been a bit worse with over 1 million deaths attributed to covid. But I can’t take the US data very seriously as the profit-driven6 health system there had too many financial incentives from government payments to be truly honest.
Almost Everything We Were Told Was A Lie
It is really hard to escape the conclusion that everything seemed to be designed to lead to a campaign of mass vaccination. I do not want to arrive at this conclusion, but everything seemed to lead, inexorably, towards vaccination - and needlessly so.
We have already seen that, at a personal level, younger people were not at any significant extra risk from covid - even based on the inflated official statistics.
The justification for vaccination of younger people, then, relies only on an assumed level of community protection that this would afford, and that it was all about protecting Granny.
It is interesting that The Great Barrington Declaration was all about protecting Granny, too. But this was deliberately, and fraudulently, dismissed as “fringe” science within days of its publication.
The Great Barrington Declaration was also put into the “let it rip” fallacy box. This is how the notion of herd immunity (an established thing, scientifically) was ridiculed and derided. In fact, it would have been a good strategy to “let it rip” amongst the younger demographic who were not at significant risk from covid. The increased level of community protection afforded by this measure, from disease-acquired immunity, would have provided a significant level of protection to Granny. This may not have been an optimal strategy, but it would have certainly been better than what we actually did.
It is also interesting that promising alternative treatments, not using expensive drugs or vaccination, were given the same aggressive dismissal. It was almost as if no solution, other than vaccination, was permitted to exist.
It was known, for example, that vitamin D deficiency was associated with worse outcomes for covid, yet where were the government advertisements recommending this very safe, very simple (and very inexpensive) prophylactic measure?
There was another factor too. The level of wholly unnecessary fear (in health terms) was critically necessary if you wanted to convince people to be vaccinated.
And yet another factor. The grotesque over-exaggeration of covid risk, promoted by psyop after psyop, meant that extremely draconian (and wholly unnecessary) ‘health’ interventions could be instigated by governments. None of these, of course, worked - and we knew they wouldn’t work. There was a reason why all previous pandemic planning had explicitly recommended against them.
Once you have these in place it is easy, then, to portray vaccines as the ‘only way out’ of all of these terrible restrictions. It becomes not just about being saved from a disease, but about being saved from a set of tyrannical ‘health’ measures that had been deemed ‘necessary’ because of the severity of the virus.
In health terms there was no justification for the draconian measures; and they knew it. It was obvious from things like The Diamond Princess and the emerging data from Italy that we were NOT dealing with some health disaster of unprecedented proportions. Moderately serious, maybe. But global ‘emergency’ level? Fornicate thyself right off, good Sir.
We knew this from almost the earliest days of the ‘pandemic’ and yet everywhere, with a few rare exceptions like Sweden, went covid crazy.
The grotesque over-exaggeration of the severity of covid was the first lie. It is like Sauron’s Ring; the one lie to rule them all.
It is only with this first lie firmly established can all the rest of the craziness be imposed.
If the first enabling lie can be described as Sauron’s baby, then the second critical enabling lie surely belongs to the Witch King of Angmar.
This lie was the myth of asymptomatic transmission (AT).
This lie was absolutely critical.
This is what convinced people, along with the severity lie, to stay indoors, to wear masks, to follow one way signs in those shops deemed to be ‘essential’, and so on. Everyone was considered to be a danger with or without symptoms. We turned perfectly healthy people, who presented no threat whatsoever, into perceived biohazards.
Yet it was based on the flimsiest of evidence - and there’s still no good evidence for it having played any significant role in the pandemic. It will have had some impact because pre-symptomatic transmission, which cannot be distinguished from asymptomatic transmission until after symptoms develop, is possible.
With the lies of extreme severity and AT in place you can ‘nudge’ people to behave in very stupid ways. I hate the word ‘nudge’ as it has been applied to the level of covid psyop we were exposed to. It implies a mild, gentle, shove in a particular direction when, in fact, it was more like being hit with a fucking sledgehammer.
The lies kept on coming. Fomite (surface) transmission was said to be significant which led to a veritable orgy of OCD-like behaviour as people religiously and frequently scraped several layers of skin off their hands with some chemical gloop called ‘sanitizer’, or rather illogically wore gloves, or doused their groceries in bleach. We even had libraries ‘quarantining’ books just in case you caught covid from one of them. Fuck me, we went crazy, didn’t we?
Don’t read “To Kill a Mockingbird” - that one tested positive for covid only just yesterday.

Whilst not initially a lie, the whole raison d'être for lockdowns quickly morphed into one. Initially we were told that lockdown was to “flatten the curve”, to slow things down so that health services are not overwhelmed, which is at least plausible. It quickly became about “saving lives” instead - which didn’t make any sense.
But, of course, it then developed into something like - just lockdown a bit more until the vaccine comes along to save us.
And then we had masks.
Oh, dearie, dearie me.
What, to steal Rikard’s lovely spoonerism, an absolute flustercluck.
I don’t want to say too much about masks; we all know they don’t work. I say ‘all’, but there are some deluded fools who still cling to these useless objects like some kind of religious talisman.
To summarize the Science™ : never in the field of human investigation has so much utter crap been written about something so patently useless.
To summarize the science : they’re shit
In the country I was living in at the time of the first year of covid I had no choice but to wear a mask. All they ever did for me was to make it really difficult to understand people and to make it more difficult to breathe comfortably. Oh, they also gave me nosebleeds. I estimated there being about a 30% chance of me bleeding all over the fresh veg section in the supermarket by the end of it all.
When I was able to ditch the mask on return to the UK, the nosebleeds went away.
Then we had (anti) social distancing. Another evidence-free imposition for our supposed ‘benefit’. They knew it was just made up shit.
I will briefly apologize here. I’ve gone from approximately professional language style to decidedly non-professional. The more I write, the more I’m reminded of the gargantuan gibberish that was deliberately imposed upon us, and the angrier I get.
Everything was so frenzied, so damaging and, ultimately, pointless. None of the interventions actually worked in any appreciably noticeable way.
I suppose we can afford a certain time period of confusion. Politicians, after all, can be as duped as the rest of us by technical gee-whizzery. They can panic too - particularly when they deem votes to be at stake. It’s probably the only time they do panic.
But as the data piled up and it became clearer and clearer that we were NOT facing this farcical global ‘emergency’ we should have had a course-correction. We did not; they doubled down and kept on making things worse.
It became all about the ‘vaccines’.
I’m getting the “too long for email” message pop up. So it’s probably a good time to call a halt for now. I want to carry on, though, because there are lots more things to cover. Testing, vaccines, immunity, the question of whether it is all best explained by conspiracy or confusion, to name a few.
I will endeavour to continue but, for now, I need a brandy.
For example, not treating with anti-virals in the early stages, or antibiotics to combat secondary pneumonia in the later stages. Or the use of ventilators or midazolam.
There are experiments in which people (volunteers) were exposed to viruses and it proved, unexpectedly, rather difficult to infect them.
I haven’t personally checked this, but I think it’s correct.
Although we did have attempts to paint covid as a terribly racist disease because it affected the noble BIPOC more than dastardly whitey, apparently.
There was a point where it was extremely difficult to confirm any re-infections. Re-infections only became more common after the vaccination programs had gotten underway. One may find that interesting, as I do.
To be fair, it’s hard to see how health provision can entirely avoid any profit motive. Should the manufacturers of MRI machines, for example, not be allowed to make a profit? The difficulty, as it so often is, is in getting the balance right. How do we get the balance right so that the profit motive (which is necessary) does not skew things against the patient?
I can relate to ‘the more I write the angrier I get’.
It’s like everything to do with the plandamic, the more i read, talk, listen, watch the angrier I get.
Yesterday my daughter told me there is a “boy”* in one of her classes who still wears a mask. “I think it’s for fashion,” she explained.
(*by “boy” we mean “girl” who has been infected by the transvirus.)