

To vaxx, or not to vaxx, that is the question
A letter I penned to my daughter's friend

I’m re-posting here a letter I wrote. My daughter asked, on behalf of a friend (let’s call her Alice) for some background information. Alice’s boyfriend (around age 30) is thinking about getting vaccinated, but Alice, who does not want the vaccine herself, is worried for him.
I don’t know Alice’s boyfriend. I know Alice a little - and she has a technical background and degree (some sort of neuroscience degree I understand). I’ve tried to be as balanced and objective as I can here and even downplay some of my concerns. I thought the letter might be useful as a kind of overview of some things - or at least my understanding of them.
Dear Alice,
XXXXX (my daughter) passed on your message asking for some background context to help you guys come to a sensible decision.
I have seen lots of forum posts with people in similar situations – the two partners are at opposite ends of the spectrum on covid. It has caused a lot of friction, and worry – on both sides. Given the level of hysteria (again on both sides) and misinformation (both sides) it’s an understandable, but invidious, position to be in.
One thing I would say is that personal choice, whatever it is, must be respected. I want my decision NOT to have the vaccine, at 56 and being a bit blobby, to be respected. I am probably on the cusp of any risk/benefit analysis here – but the long-term unknowns sway it for me. If someone comes to an opposite decision – that’s fine.
That doesn’t mean we wouldn’t worry about someone who comes to a different decision to us. It’s not easy.
Just how Dangerous is Covid19?
I’m going to put the figures here for deaths up to 9th April 2021 for England & Wales. This was as the second season (or “wave”) had petered out and we were coming into the very low impact Summer season (all coronaviruses show this strong Winter/Summer seasonality in temperate regions – why this is, is not properly understood – but it is widely known)
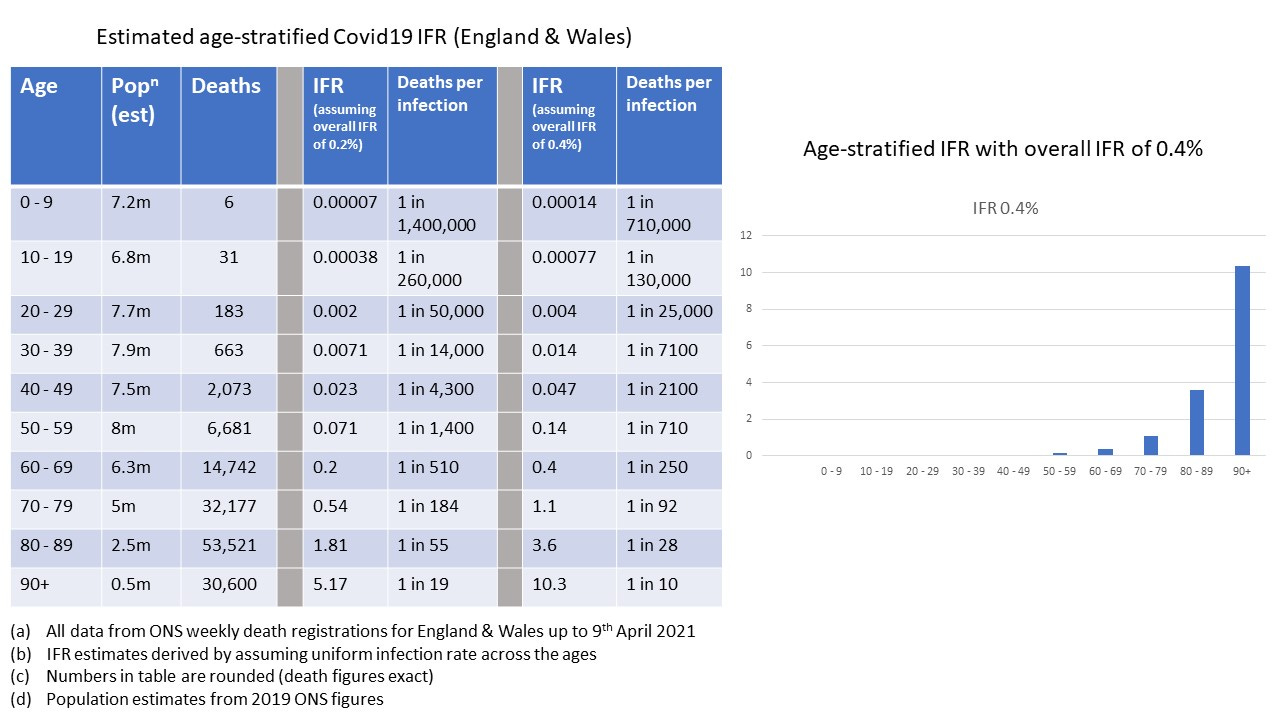
If we just accept the raw figures at face value we would conclude that a reasonable estimate of risk for someone at age 30 is about 1 death for every 10,000 infections.
However, these figures are actually upper bounds. The process and methodology for recording of death was changed during the pandemic. Deaths, for any reason, within 28 days of a positive test were classed as a “covid death”. The figures are thus an overestimate of both deaths and risks. This change of recording is difficult to understand because it leads to the opposite of what we need – we need accurate statistics in order to determine the severity and the best actions to take.
The other thing that is really important to understand is why people die of covid19. It overwhelmingly seriously affects people who have, for some reason, a compromised or sluggish immune system. The figures in the above table are overall figures. We know that the people dying are overwhelmingly those with some other health issues that have an impact on immuno-efficiency.
So for a healthy person at age 30 you’re looking, conservatively, at a risk of death around the 1 in 40,000 infections level.
Why do people die of covid19?
I’m not an immunologist, or clinician, but I have spoken to those who are – and this is my current best understanding.
In general there seem to be 3 distinct phases of disease progression. It starts off as a respiratory infection similar to flu. This is where it stops for the vast majority, if it even goes beyond mild symptoms at all. If you’re unlucky, or more immune-compromised, then it can progress to the 2nd stage where it presents more as an inflammatory vascular/blood disorder. Thankfully, most survive this stage too. If you’re even more unlucky, or even more immuno-compromised, then the 3rd stage is essentially a thrombotic condition where the body and organs are overwhelmed by micro-clotting events brought on by a vicious immune response.
It sounds paradoxical to say immuno-compromised on the one hand – and on the other to ascribe the very serious disease to a massive immune response. But this actually makes sense.
Usually with a respiratory virus the infection is dealt with in the nose and throat – the mucosal antibody and T-cell response being important here. If this stage is not successful the virus continues to replicate and can start attacking other areas of the body. The body is still fighting it off, but now there is LOTS more virus about. The immune system kicks up a gear – and kills infected cells. It is this that causes the inflammatory response.
So if you don’t deal with the virus quickly enough (sluggish immune response) the virus can very quickly get out of control in the body (exponential growth). The body then needs to mount a massive immune response – and that can be dangerous. By the time the immune system really kicks in, the virus is everywhere and the immune system kills off the body’s own infected cells.
This is why early treatment is so very important – get things under control before the virus replication goes into overdrive. This has been the standard clinical approach for other respiratory infections, but it has proven problematic with covid for what are largely political and financial reasons.
Young people, and kids in particular, don’t tend to have any problems with the speed of their own immune system – and so the virus is quickly and effectively dealt with. Note also that this is why kids are not good vectors of transmission – the virus is dealt with before they are even able to shed any significant viral load to others.
The elderly immuno-senescent and immuno-compromised are shedding orders of magnitude more viral load because the virus has been able to progress further (exponential growth again).
So, what about the vaccines?
The first thing to note is that if you have already had covid, there is no need at all to be vaccinated. The natural, infection-acquired, protection this affords is longer-lasting and at least as effective as that of the vaccine – lots of work showing this now. Indeed, many studies have shown that natural immunity is significantly better. There are also some concerning studies which are showing that the vaccine doesn’t “top up” natural, infection acquired, immunity – but actually interferes and damages the existing natural, infection-acquired, immunity.
Of course, some of these conclusions are provisional – but a fairly consistent pattern is emerging. You may see a lot of studies showing that antibody levels are much higher after vaccination – using antibody level as a proxy for effectiveness. But it doesn’t follow at all that a massively disproportionate level of antibody is necessarily better (think about Vitamins here – taking a large excess doesn’t achieve much as, for most vitamins, any excess just gets flushed out).
A massively high level of a certain amount of specific antibody (to just the spike protein, for example) may even interfere with the other natural responses – which are based on several different kinds of antibodies, and also on T-cells and other mechanisms – it’s much more complicated than the naïve assumption that more spike antibody = better protection).
The other problem, particularly with “leaky” vaccines is that of Original Antigenic Sin (OAS). This is where exposure to a prior infection can lead to a maladapted response to a slightly different variant or strain. This is seen in natural infections (Dengue fever being the classic example). Essentially the body’s immune response gets primed to behave in a certain way – and when a new slightly different version of the same infection comes along, the body just relies on the old response, and doesn’t go through the process of creating a new response.
With the vaccines you create an immune response – but if this isn’t quite the right one for a new version (variant) it’s possible you’ve made things worse for yourself by vaccination.
These are concerns – a bit hypothetical – although I think we have seen some evidence of OAS happening. But what about the real-world data regarding covid vaccinations?
Here we run into all sorts of data transparency issues. The FDA in the US have asked a judge, and been granted as I understand it, to be allowed to release the full vaccine trial data at a rate of 100 pages a month. It will take 55 years for the full data to be released. I don’t see this as anything other than a gross attempt to hide something. I don’t know how to rationally interpret this in any other way.
So what does the data we have seem to say? I say “seem” here – because it really isn’t clear. With statistics you have to be really careful – all sorts of things can mess things up. For example, a professor of risk statistics has recently demonstrated that simply by introducing a 1 week delay in the statistics you can make a placebo (with 0% effectiveness) seem to have a significant benefit!
But let’s be optimistic. It would seem that vaccines do have some protective effect against serious symptoms and death. I don’t believe the government figures of 80-90% at all. There are significant numbers of double-vaccinated people in ICU with covid19 right now. The protection is not perfect and probably not high.
It also wanes. A recent Swedish study showed that the protection against symptoms had gone negative after 3-4 months. Whatever the facts – and the situation is much more confusing and cloudy than the media would have you believe – it is clear that significant number of scientists across the world have some very serious concerns.
We also see some very concerning data in the Pharma trials themselves. Yes, that data showed 90% levels of protection against symptoms (not serious symptoms or death – these were not trial endpoints) – but the data also showed that when you looked at health overall (all-cause morbidity) the vaccine recipients were actually worse off. We must also remember that the trials had a very unrepresentative (population-wise) set of trial participants – various important groups were excluded from the trial.
We’re also seeing plenty of data that contradicts the 90% effective claims of the trials. There is a very high degree of correlation between level of vaccination and increase of covid cases. We’re seeing it everywhere across the world. Vaccination has not helped at all and appears to be making things worse.
My own analyses of the ONS data have shown that there has been a very worrying trend of increasing excess overall mortality in the over 45’s over the last few months. This may be treatment delay caused by shutting down the NHS to become a covid-focused service, or it may be vaccine effects. Or both. I don’t know, but it’s very concerning. It isn’t covid because covid isn’t contributing much to overall death right now.
But even if the vaccines prove to be effective, there is the other side of the coin. The side effects. These are routinely dismissed as “coincidence” but the sheer numbers are staggering. In the UK alone, the Yellow Card system for reporting adverse vaccine effects has had over 1,730 death reports in less than a year.
The death rate for every single other vaccine combined – ALL of them combined – is an average of 8.3 reported deaths per year. All other vaccines (flu, tetanus, shingles, etc) have a combined level of reported death of 8.3 per year. And it’s not a numbers issue – in 2019 in the UK there were 15 million doses administered of the flu vaccine alone.
I simply don’t know how anyone can explain away this massive increase in reported death as mere “coincidence”. That this is done is worrying enough in itself.
If we focus just on one side effect (there are many reported side effects all tending to cluster around neuropathy/thrombotic problems) we can see indications of some very serious trouble ahead. Estimates vary, but some have put the risk of myocarditis in young men caused by the vaccine at 1 in 5,000 injections. I think that’s maybe too high, but there has been a really worrying increase in young men presenting with heart conditions (and dying on the football pitch).
Myocarditis is not trivial. It is always serious. It can be managed and can go away – but it can also significantly shorten life and quality of life. I don’t know why a young person would want to trade a 1 in 40,000 risk of dying from covid with side-effect risks at these levels by taking the vaccine. But that’s just my view – others will come to different conclusions.
I’m sorry for going on so long – but it is a very serious issue – and it is very complex – nothing like the hopelessly simplistic picture presented in the media.
I hope I’ve given you some food for thought by presenting my current understanding and view – please also seek alternative views and opinion – I might not be right, after all. There are conflicting views – but even the inventor of the mRNA vaccine technology is urging extreme caution with these covid vaccines. That’s enough, for me, to want to take a much deeper and careful look.
Well written but a tad wordy, in my opinion. If your daughter’s friend respects your opinion, she’ll likely made it through. But that would depend on her age, too, and her experience with personal electronics. Much of the youth these days have a short attention span.